Order in Chaos
“Importantly, change need not be conceptualized as the consequence of a cause destabilizing a previously stable system.” Derry, p.20
Recently I read a fascinating article, “Nonlinear dynamics and positive health: The case of menstruation/menopause.” Admittedly, the title isn’t that sexy, but the information contained within was juicy.
Essentially, the author explores the evidence for viewing menstruation and menopause as complex systems. “Consistent results were found across the multiple methods of data analysis: The menstrual cycle is characterized by chaotic dynamics rather than disorder, randomness, or linearity throughout the life cycle…” (p.16)
Why is this important?
Complex systems are those that are subject to what we think of scientifically as chaotic system dynamics. There are several properties that characterize complex systems, but those that are most pertinent to thinking about the physiological cycles women are subject to include:

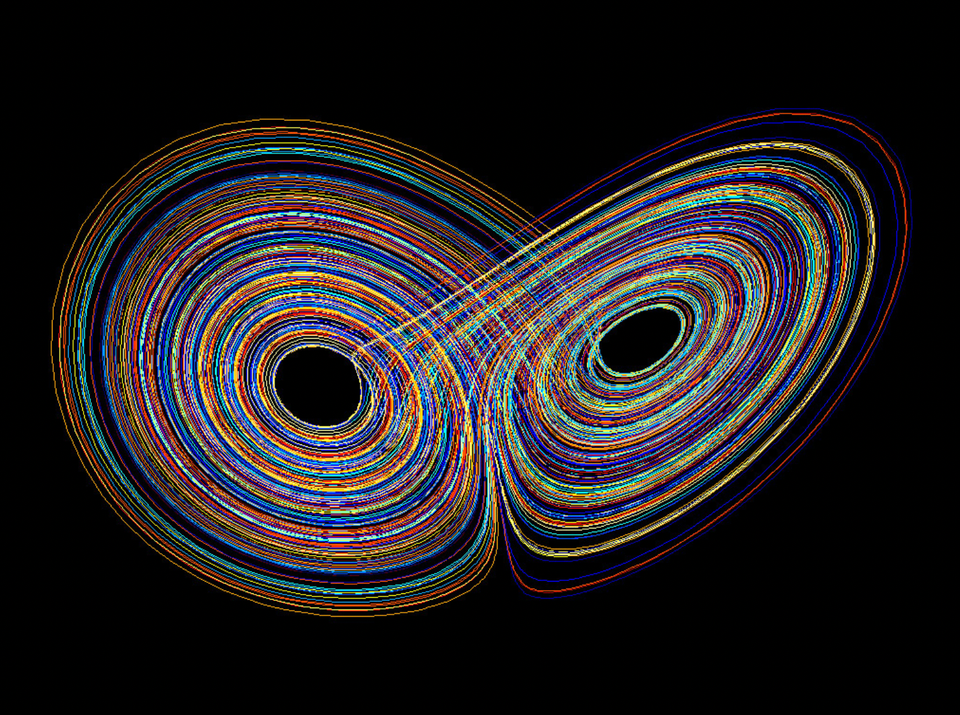
· Sensitive dependence on initial conditions: This idea is best encapsulated in the metaphor of the butterfly flapping its wings in the Philippines and catalyzing a hurricane in the Caribbean. Small shifts in one area of the system lead to vastly different outcomes along myriad trajectories and the future is unpredictable because evolution is ongoing. The butterfly wings could just as naturally lead—alternatively or simultaneously—to a mild spring in the Andes and/or increased drought in northern Africa.
This leads to the next characteristic of complex systems:
· They are deterministic, but unpredictable. As Google AI summed up this paradox, “While the behavior of a chaotic system is fully determined by its initial conditions, its sensitivity to those conditions make long-term prediction impossible.”
Here’s how I understand this with regard to menopause:
The “initial conditions” of menopause have to do with whatever mix of hormones is present in a woman as well as her baseline health in a variety of domains—physical, mental, emotional, relational, etc.—and the external circumstances of her life. However, we cannot know how the menopause transition is going to evolve or resolve for any individual person because the sensitivity of the system itself to all the constantly changing parts of the system makes it impossible to forecast accurately how things will go or how they will ultimately settle out.
Chaotic systems are also critically:
Nonlinear, Complex, Aperiodic:
· Aperiodic means that complex systems do not typically settle into repeating patterns or cycles. But doesn’t menstruation do exactly that? Derry, the author of the article, suggests that perhaps it doesn’t. Or at least that it doesn’t to the extent that the medical field would like to imagine it does. As she writes, “the menstrual system is the right kind of system to have chaotic dynamics: multiple systems of control with bidirectional feedback loops” (p.14).
o One 2022 study done through the Harvard T.H. Chan School of Public Health found that menstrual cycles typically vary 4-11 days among women depending on age, health, BMI, etc. And this is the variation found among women in one study. What about the variation one woman alone may experience in a lifetime of menstrual cycles affected by travel, emotions, pregnancy and breastfeeding, illness, etc.?
o Certainly, menopause may offer itself as the very definition of aperiodic, a system that has been fairly reliable—even in its variability—that suddenly becomes quite chaotic and unpredictable.
· Complexity as a characteristic of chaotic systems means that these systems can exhibit intricate and complex patterns. So while there is, perhaps, a lack of rhythm or predictability in what is happening in the day to day, there may be a larger pattern forming that could be seen if we can move ourselves to a different vantage point in time or space. The possibility exists that what seems crazy, chaotic, scary, and/or frustrating in the immediate experience of menopause could be a natural and completely appropriate unfolding of change within the unrecognized wisdom of a complex system.
· Critically, complex/chaotic systems are Nonlinear. Unfortunately for women, or anyone whose bodymind does not conform to simple cause and effect logic (i.e., every body), our healthcare system and how we view bodies through the lens of that system, is based on linear models--input and output, catalyst and reaction.
o We have cultivated and maintained this linearity of thought quite consciously and unconscionably. As already noted elsewhere in this blog, for decades women have been excluded from medical trials and experiments because it was quite openly acknowledged that the complexity of their physiology would complicate the results. Even today, women, People of Color, and people of varying gender expression continue to be excluded from health exploration because their bodies challenge the reductionistic views required by the linear model.
For the time being, I don’t really want to focus on the injustice of being caught with
· a complex system—a woman’s (or gender diverse) body—
· at a sensitive time—menopause (or always)—
· within a linear system of thought and behavior—the American (or Western) healthcare system
Instead, I just want to share a few points from Derry’s research that I found helpful when thinking about how to recontextualize menopause so that, in all its chaos, craziness, fluctuation, unpredictability, and uncertainty, it can be viewed as absolutely normal, a part of life no stranger than the shifting of tectonic plates, the emergence of new life forms, or quantum physics.

I. “Variability and unpredictability can define a healthy rather than an unhealthy system.” (p.24)
· In her paper Derry makes an important point: Data is read differently in linear systems than in complex systems. In linear systems, “means, standard deviations, and other measures of central tendency are regarded as accurate representations of collective data and often conflated with the ‘real’ results, often representing the optimal or normal…” (p.4). Variability, especially in the form of outliers—those data points that lay furthest from the average—is considered aberrant or “noise.”
o Consider how many times in your own life you have found your body behaving outside of its own “normal.” Think about all the different emotions, situations, or events that have had an effect on your physical and mental health in general and your menstrual cycle in particular. And then, imagine where you might find yourself on the great bell curve of aggregated data gleaned from women menstruating all over the world. Would you be “normal”? Or are you more likely to be “noise”?
· Linear models tend to “proceed from the assumption of reductionism” (p.25). That is, they break the system they are looking at into separate parts and view these separate parts as having distinct roles to play, reasons for being, and effects to produce. When hot flashes and rage spikes are reduced to the “cause” of low estrogen, the linear model’s response is to input more estrogen and assume that that will “effect” a cure. In complex/chaotic systems, this approach may be effective. However, it is just as likely that introducing more estrogen will actually create more chaos. Indeed, not many decades ago, introducing estrogen into the system of a woman who still had a uterus put her at greater risk of contracting uterine and endometrial cancer. It turns out that we also needed to introduce progesterone to counter the impact of estrogen on the uterus.
o Apart from the fact that simply prescribing estrogen to a sweaty, sleep-deprived woman may be akin to putting some oil in the engine of a cranky high-end sports car and expecting it to start purring again, when we reduce people to “problems” and attempt to apply algorithm-based “solutions,” then “this discourages considering whether problems and distress are complications of menopause whose cause and remediation need further investigation” (p.22).
I personally have needed the following interventions in order to wrest health, psychological well-being, meaning, and order from my menopause transition:
· HRT—estrogen, progesterone, testosterone, vaginal DHEA
· Sleeping meds
· Psychotropic meds (mood stabilizers)
· Dietary changes
· Supplements
· Bodywork (massage, acupuncture, chiropractic)
· Exercise (strength training, yoga, swimming)
· Talk psychotherapy
· Couples counseling
· MDMA-assisted psychotherapy
· Yoga teacher training
· Women’s health coach training
· Participation in a year-long writing program
· Ongoing support and connection with friends
We are a complex system with multiple intertwined components that are always in motion and changing in relationship with each other. Viewing ourselves as a static collection of separate parts like tools lined up on a workbench makes absolutely no fucking sense.
II. “Stories and language can encourage or discourage a sense of meaning, feeling empowered or helpless, a sense of well-being.” (p.11)
How we view our bodies is impacted by our being contextualized within a linear system of thought.
· When we rely on averages and norms from aggregated and reductionistic data, we start to understand our own experience by comparing it with external standards or, as Derry puts it, “objectifying one’s body as an object of scrutiny” (p.20).
· If we do not understand that variability and unpredictability are an inherent and natural part of our complex systems, then we tend to “monitor” ourselves for changes. This tends to encourage “an alienated stance toward the body” (p.23) and we are more likely to view symptoms and experiences that fall outside the range of the “norm” with anxiety, vigilance, and uncertainty. This, in turn, encourages us to continue to seek outside ourselves for “treatment” for what the linear paradigm describes to us as illness.
· The ”value-laden language” of linear systems used to describe menopause affects our ideas about ourselves, our bodies, and how we relate with our experiences:
o “resistant” ovaries
o “erratic” hormones
o “abnormal” cycles
o “senescence and/or pathology in which an unstable and disordered system no longer responds normally to hormonal and other signals”
Derry writes, “Indeed, the World Health Organization (WHO, 1996) definition of menopause is the cessation of menstruation associated with the loss of ovarian function—'loss,’ not ‘change’ or ‘completion’” (p.13-14).
Viewing ourselves and our menopause transitions instead through the lens of a complex systems perspective
· Allows us to embrace variability and unpredictability
· Encompasses a broader array and variety of experiences into what is natural and healthy
· Encourages each woman to stay current with and interested in her own experience rather than comparing herself externally to dubious norms or other unique individual processes
· Helps cultivate awareness of things we are experiencing that are interesting, enjoyable, feel good, and seem important, not just the things that are going wrong or feel bad, or missing things that remain invisible simply because they don’t register on the mainstream’s radar.
The most critical aspects of any single person’s menopause experience are likely to be outliers in any mainstream data set. It won’t show up in the literature, on the pamphlet in the doctor’s office, or even on a podcast for women by women! You won’t see it if you aren’t tuned in to yourself.
Derry writes, “If the task is to understand one’s unique pathway, then, in addition to gathering information from expert sources, information is needed about one’s own experience” (p.21).

III. “A complexity perspective on the underlying physiology is consistent with existing theories that regard menopause as part of a life stage of healthy post-reproductive adulthood rather than health-threatening aging.” (p.25)
· Because human women typically live for decades in a post-reproductive state, and well before other body systems begin to significantly age and decline, it makes sense to consider the possibility that menopause may offer us a unique stage of biopsychospiritual evolution that, in fact, “involves a stretching out of the time that the stage exists…a slowing down of aging or a life stage before old age” (p. 25).
· I have pointed out that in her podcast interview with Andrew Huberman women’s exercise physiologist Stacy Sims described women’s experience of the aging process as “falling off a cliff,” and that has, indeed, been my personal experience of the perimenopausal transition. However, I think Derry is also onto something, particularly if we are seeking to understand and embrace the opportunity and benefits the menopause transition offers.
· The changes wrought by perimenopause are often abrupt, chaotic, and unpleasant. They tend to delineate a stark demarcation for a woman between her identity before and after the changes comprising “The Change” take place. However, because menopause shifts us directly into a state of freedom that is unique within our lifespan—freedom from cycles of fluctuating inner states (emotionally and physically) as well as freedom from potential reproductive imperatives—we are also presented with a space of time in which we can still be healthy, strong, vital, and creative in ways that are novel to us and potentially radical for society.

Menopause does mark a transition into a state of greater physiological vulnerability. With the natural decline of estrogen, progesterone, and testosterone in our bodies the reality is that our organs, muscles, skin, and bones are at greater risk of illness and injury. However, it is also true that we have choices about how we engage with this vulnerability physically, psychologically, and emotionally. The personal choices we make about
· The meaning of menopause
· Our worth as women
· What kinds of foods we eat and drink
· How and how often we move our bodies
· Sleep
· Our relationships
· The work we do
· How to treat and/or fortify our bodies—supplements, hormone therapy, pharmaceuticals
· Where we live
· How we live and behave toward others
among many other choices, are likely to have an impact on how rapidly we age and decline. The societal or communal choices we make about all of these things impact each of us collectively and individually as well.
I have offered these ideas and musings on menopause as a complex/chaotic systems process because it has helped me to appreciate both the profound complexity and wisdom inherent in women’s natural physiological transitions as well as the forces that work against us understanding these transitions as both natural and wise. I hope you find it both interesting and helpful as well.
References
Derry, P. (2022). Nonlinear Dynamics and Positive Health: The Case of Menstruation and Menopause. Nonlinear Dynamics, Psychology, and Life Sciences, 26(3), 237-258. https://static1.squarespace.com/static/515dcfebe4b0bca14d7919a7/t/6373b979d3122215bc5e6dbe/1668528505977/Complexity+Positive+Health+Meno+final+version+to+share.pdf
Harvard T.H. Chan School of Public Health. (2022, November). Menstrual cycles today: how menstrual cycles vary by age, weight, race, and ethnicity. https://hsph.harvard.edu/research/apple-womens-health-study/study-updates/menstrual-cycles-today-how-menstrual-cycles-vary-by-age-weight-race-and-ethnicity/
Image References:
Lorenz Attractor: https://projectnile.in/2021/07/24/quantifying-the-patterns-of-chaos/
Square waves: https://www.surfer.com/news/square-waves
Body Politic: https://www.symphonyspace.org/events/vp-the-body-politic-an-evening-of-live-storytelling
Print Gallery, Escher: https://medium.com/@annabelle_67699/philosophical-and-literary-themes-in-mc-eschers-print-gallery-f073cf2324d4